

Previous
What and why: introduction and principles

In its simplest form, Job Planning is a system of identifying and allocating time in a proportioned way for each clinician to activity broadly categorised as:
|
|
Clinical careSeeing patients and all the associated work included in that care such as notes, reports and indirect contacts, as well as supporting the wider population through the provision of Population Health activity. This aligns with the Clinical Practice Pillar. |
|
|
Supporting Professional ActivityAll the activity required to be a competent and well supported clinician, aligning with the three Pillars of Facilitating Learning, Leadership and Service Improvement/Evidence, Research and Development. For example Continuing Professional Development, mandatory training, supervision and participation in service development, as well as other role specific duties such as operational management. This also includes other activities such as staff side representatives and the day to day running of a service. |
Each member of the team has a Job Plan which reflects what they do in their role, which relates to their career and service goals, and which they have ownership of (Allied Health Professions—education and workforce policy review: recommendations—gov.scot). How Job Planning relates to policy can be explored further in the Job planning and policy section of this resource.
Proportioning and allocating time for each staff member to both Clinical Care and SPA can support workload management and allow capacity to participate in all four Pillars of Practice. This can help identify any imbalances or gaps in their Job Plan. Clinical time can then be allocated to clinical activity, with time for Facilitating Learning, Leadership, Service Improvement, Evidence, research and Development as well as other non-clinical activities.
Job Planning can help to support challenges faced by AHP services such as:
Collectively, individual Job Plans allow services to represent capacity in a more meaningful way. For example, a service can now identify service capacity as follows:
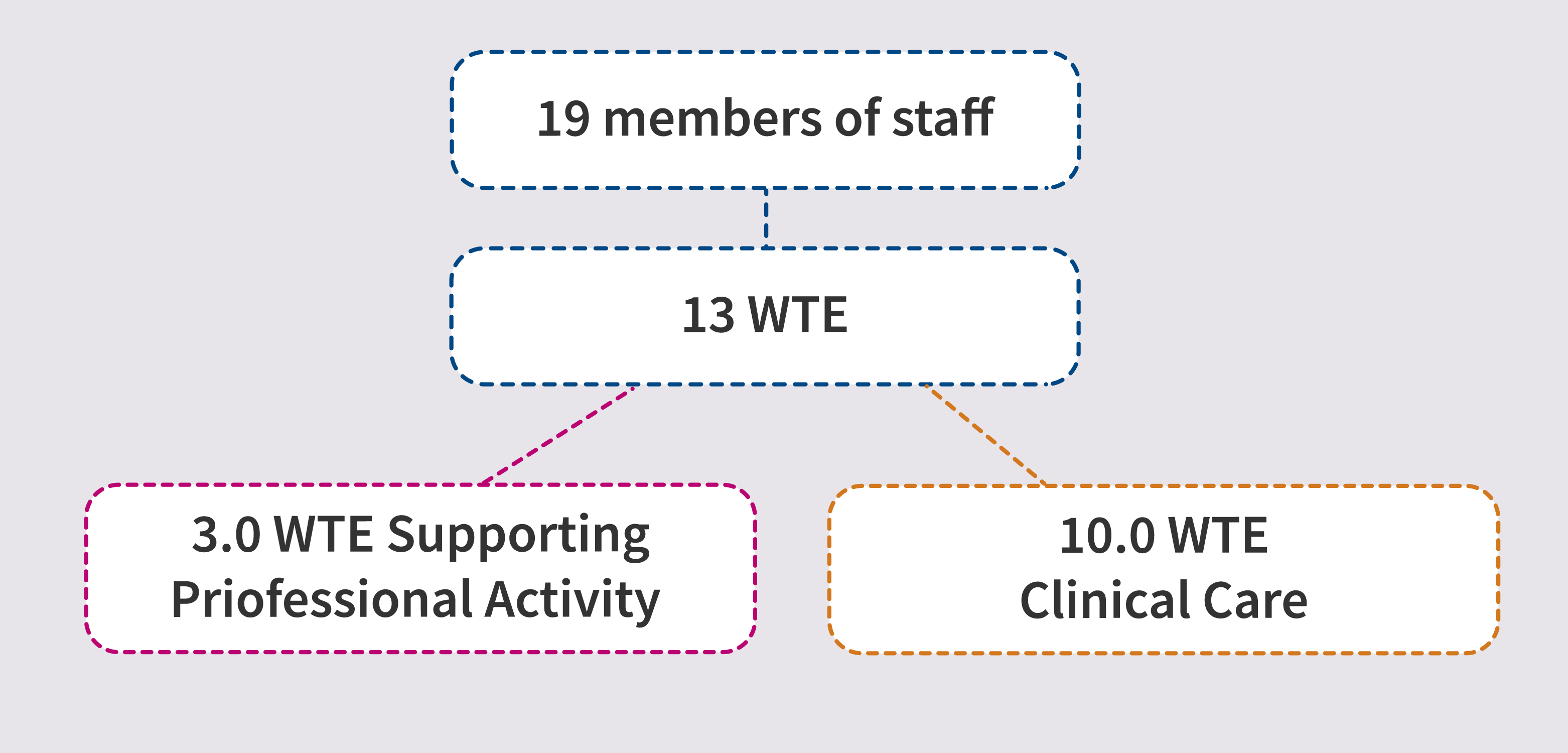
This diagram shows that the service is made up of 19 members of staff, however many are part time therefore this equates to 13 whole time equivalents (WTE). Of that, 3.0 WTE worth of time is allocated across the team to Supporting Professional Activity. This then equates to 10.0 WTE worth of clinical time.
Being able to identify capacity in this way gives a more realistic representation of the capacity within a service to deliver Clinical Care.